
This is a common question asked by my CKD patients when I prescribe them cardio-protective medication like cholesterol-lowering medicines(Atorvastatin/Rosuvastatin etc) and blood thinners(Aspirin/Clopidogrel).
Chronic Kidney disease patients many times have risk factors for heart disease like – diabetes, hypertension, obesity, smoking, advanced age, etc. There are prediction models or formulas to calculate an individual’s risk of getting a heart attack over the next 10 years. This ASCVD risk assessment if predicts a 10-year probability of CV event to be >10% then it is worth starting on this cardioprotective medication. But these risk prediction models or formulas do not have kidney function as a factor in them, because Kidney disease independently is a major risk factor for heart-related events.
50% of CKD patients never reach the stage of dialysis, as they succumb to a heart attack. The uremic toxins that accumulate in the body because of impaired clearance by poorly functioning kidneys contribute to vascular inflammation and progressive atherosclerotic disease and hence increase heart-related events in CKD patients.
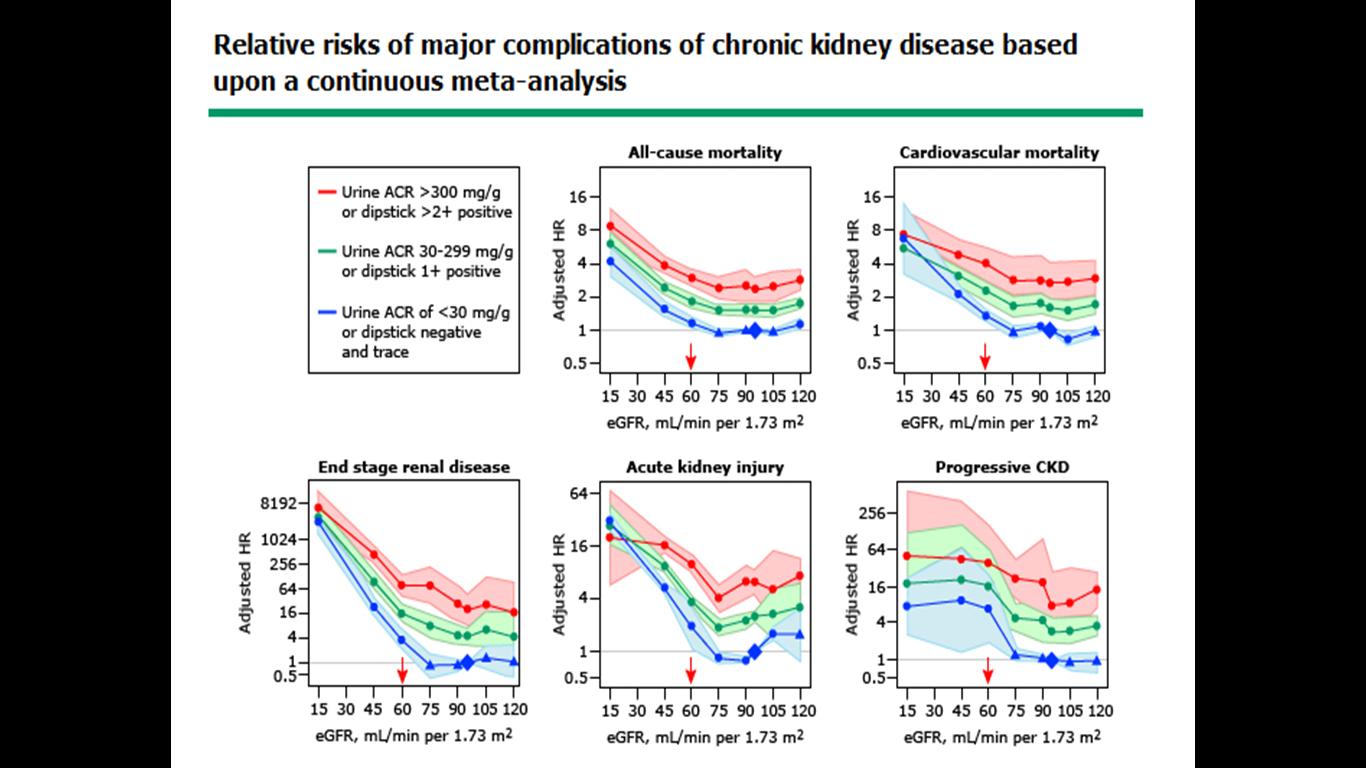
Looking at these graphs it suggests that those who have increased Urinary albumin in the Urine(Green and Red lines), even if they have normal kidney function eGFR(60-120) they are at a 2-4 FOLD increased risk of dying due to a Heart-related event(Cardiovascular mortality) and when the kidney function (eGFR)starts to decline( eGFR below 60) then this risk steeply increases.
Hence it is advisable for all CKD patients who either have Urine albumin above 30 or eGFR<60, to be on cardioprotective medications like Aspirin or Clopidogrel and Atorvastatin.
Article by
Best nephrologist in Hyderabad
Your material is amazingly unique.